The Growing Ebola Outbreak in the Democratic Republic of Congo
The Democratic Republic of Congo (DRC) is currently facing a significant rise in Ebola cases, with nearly 600 confirmed infections and over 130 deaths reported. This outbreak, caused by the Bundibugyo strain of the virus, presents unique challenges for health authorities and communities alike.
Ebola is a rare but severe viral disease that initially causes symptoms such as fever, fatigue, and muscle pain. As the infection progresses, it can lead to vomiting, diarrhea, and internal bleeding, which may manifest as blood in vomit or feces, as well as bleeding from various parts of the body including the nose, gums, vagina, and puncture sites.
The virus spreads primarily through direct contact with bodily fluids such as blood, faeces, and vomit. It can also be transmitted through contaminated surfaces or contact with the bodies of those who have died from the disease. However, transmission without direct contact is not common.
This current outbreak was first confirmed on May 15, with an estimated 246 cases at the time. However, as surveillance efforts increased, it became clear that the outbreak was much larger, with cases spreading to Uganda as well.
Understanding the Spread and Challenges
One of the key factors contributing to the rapid spread of the virus is its long incubation period, which can last between two to three weeks or even longer. This means that the number of infected individuals has likely been growing since at least March or April.
Early warning systems like Epiwatch detected signals of unknown illness in the DRC as early as April 13, with reports of hemorrhagic fever noted even earlier on March 13. However, the delay in diagnosing Ebola may have been due to initial testing targeting the more common Zaire strain, rather than the specific Bundibugyo strain.
In addition to the Ebola outbreak, the DRC is also experiencing other serious public health crises, including mpox, measles, malnutrition, and chronic malaria. These underlying conditions can complicate epidemic management and make detection more difficult.
Lessons from Past Outbreaks
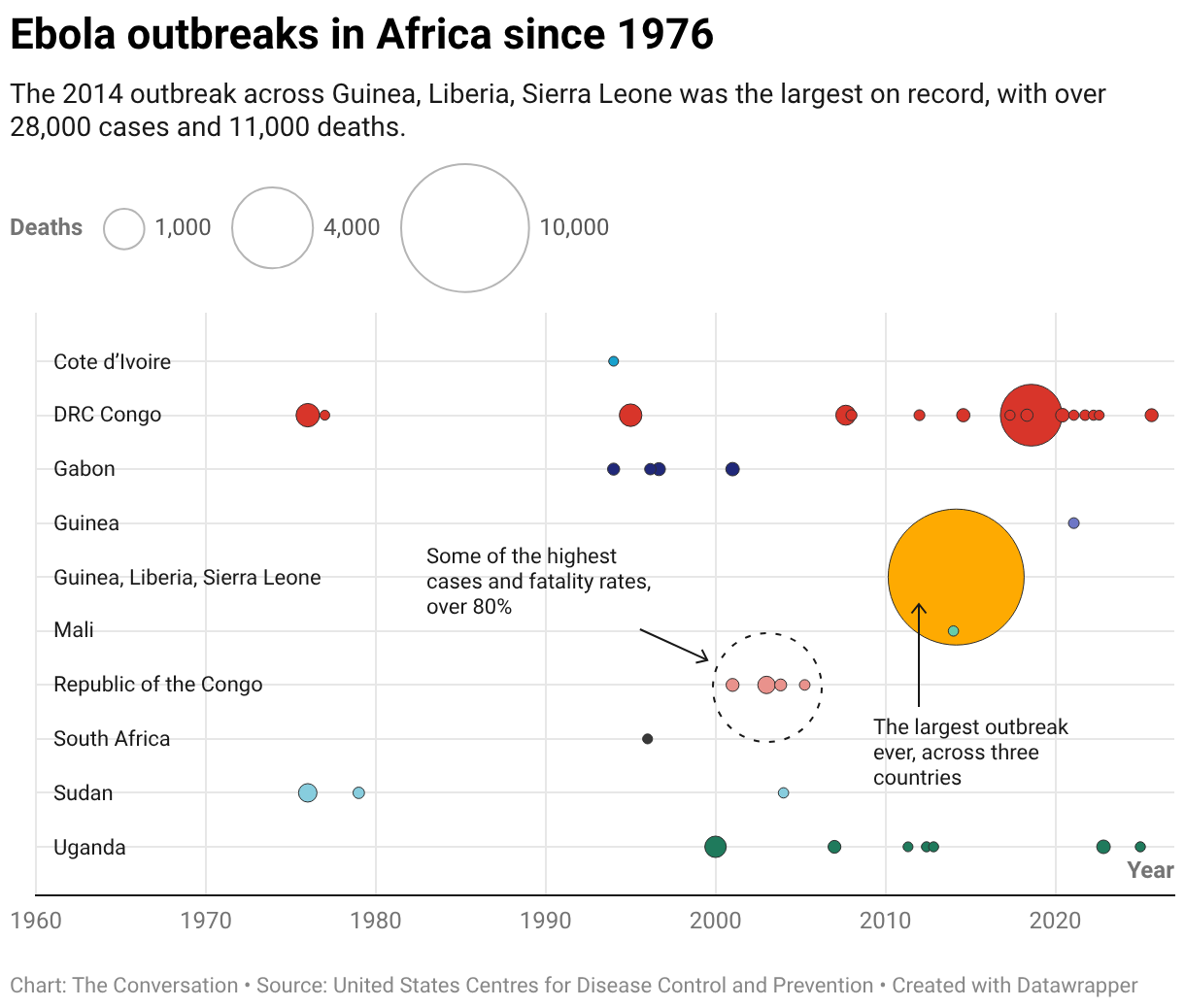
The worst Ebola epidemic in history occurred in West Africa in 2014, with over 28,000 cases and more than 11,000 deaths. At the time, no vaccines were available, but containment measures such as identifying cases, isolating patients, and tracing contacts helped bring the outbreak under control.
In the DRC, the last known Ebola outbreak was in late 2025, with only 64 cases. The largest outbreak in the country occurred between 2018 and 2019, with over 3,000 cases. Both of these outbreaks involved the Zaire strain of the virus.
There have only been two previous outbreaks of the Bundibugyo strain. The first, in 2007, had 149 cases in Uganda, near the DRC border. The second, in 2012, had 57 cases in the DRC. The current outbreak is already the largest in history for this strain.
While the Bundibugyo strain is less lethal than the Zaire strain, it can still kill 30–50% of those infected. In this outbreak, the fatality rate appears close to 30%, with 139 deaths reported from nearly 600 cases.
Unlike the Zaire strain, there are currently no approved drugs or vaccines for the Bundibugyo strain. However, the World Health Organization is sponsoring clinical trials of a monoclonal antibody and the antiviral remdesivir, which is also used for treating COVID-19.
Containing the Outbreak
Containing the outbreak requires coordinated surveillance and containment measures. This includes identifying cases, isolating them to prevent further spread, tracing their contacts, and quarantining those at risk.
In 2014, similar measures helped control the Ebola epidemic despite the lack of treatments or vaccines. This highlights the importance of strong health system capacity in managing outbreaks.
During the 2014 epidemic, hospitals lacked enough beds for Ebola patients, so tent hospitals were built to help manage the crisis. This approach could be considered if hospitals become overwhelmed during this outbreak.
The DRC has limited capacity to diagnose Ebola, so scaling up surveillance and testing is crucial. A clinical case definition, such as “fever and bleeding means a probable case,” can be used when testing is not available.
Simple surveillance systems, such as open-source intelligence, can also help detect early signs of epidemics. Providing incentives for communities to report suspected cases can further support these efforts.
Engaging Communities
It is essential to communicate and work with communities and local leaders from the ground up. In the 2014 epidemic, locals murdered eight Ebola workers who provided health education, highlighting the importance of trust and community relationships.
Health workers, close contacts of patients, and funeral attendants are at high risk of infection. They must take extra precautions to protect themselves.
Global Implications
Ebola is a concern for all countries, as travel can lead to infections occurring anywhere. During the 2014 West African epidemic, cases were reported outside the main affected countries, with the largest number in Nigeria.
Failure to diagnose a case in Texas led to four additional infections, including among health workers. This underscores the need for emergency departments to improve their awareness of infectious diseases and their ability to prevent hospital outbreaks.
Tools such as decision-support systems used during triage can prompt staff to ask about a patient’s travel history and provide data on disease outbreaks in the country of travel. This helps ensure that patients with deadly infections are isolated before they can infect others.
Another concern is that survivors of the virus may still carry the virus in their bodily fluids for months or even years after recovery. If they come into contact with others, they could continue to spread the virus.
The WHO declaring a public health emergency of international concern activates additional measures and resources to help control the outbreak.





