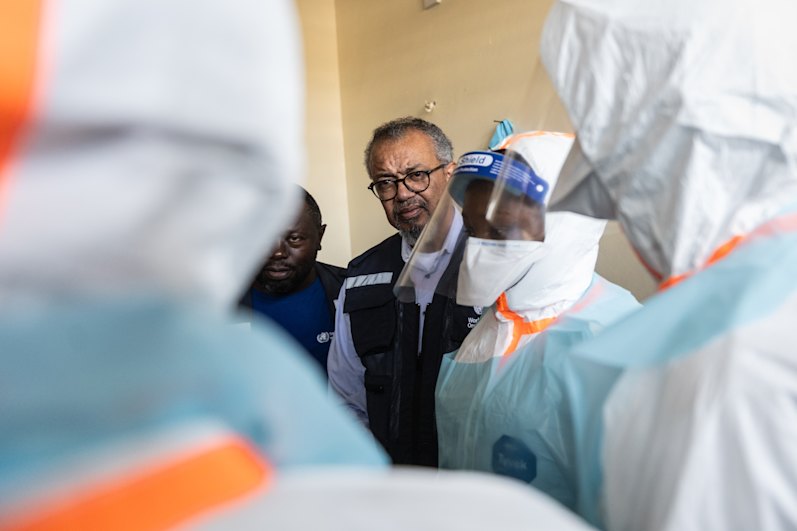
Jane Halton found herself in a critical room with global health leaders as the World Health Organisation issued its most severe warning regarding the escalating Ebola outbreak. The meeting, held on the sidelines of the World Health Assembly in Geneva, included none other than WHO Director-General Dr Tedros Adhanom Ghebreyesus, who had just declared the burgeoning epidemic in the Democratic Republic of the Congo (DRC) a Public Health Emergency of International Concern. Amidst the gravity of the situation, Dr Tedros’s phone was a constant source of urgent updates.

“Terribly, in the course of that meeting, Tedros was getting text messages from WHO people on the ground who were actually being fired on in their tent,” Halton recounted, recalling the May gathering. “It’s a very dangerous part of the world.” Halton’s extensive career in public health, including her tenure as the head of the Australian Health Department from 2002 to 2014, and her involvement in Australia’s pandemic response through the National COVID-19 Co-ordination Commission, provided her with a unique perspective. Her influence expanded globally when she assumed the chairmanship of the Coalition for Epidemic Preparedness Innovations (CEPI). This vital alliance, comprised of governmental bodies, scientific institutions, and civil organisations, was established in the wake of the unprecedented Ebola outbreak that began in 2014. That devastating epidemic saw 28,600 infections and 11,325 fatalities across West Africa.



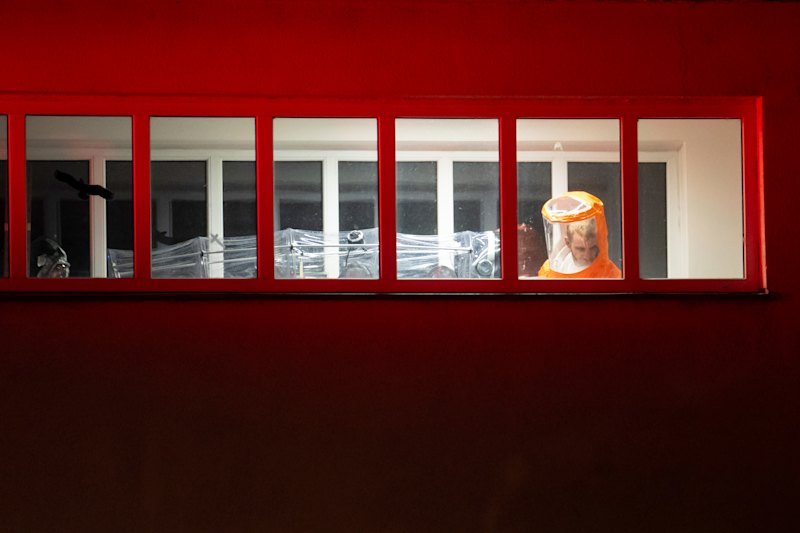
The current outbreak, some experts fear, could potentially rival the scale of that past disaster. As of June 7, there have been 569 confirmed cases and 103 deaths reported across the DRC and Uganda. Modelling suggests that the actual number of cases could be double the reported figures. Dr Tedros himself warned recently that the disease may have been circulating undetected for as long as four months, spreading through bodily fluids, including blood, vomit, and semen, before the official outbreak announcement on May 15. The region is grappling with a rare strain of the Bundibugyo virus, for which no vaccine or established treatment currently exists. Compounding these challenges, the area is plagued by inter-militia violence, and the spread of misinformation only exacerbates the dangerous situation. In some tragic instances, medical tents have been set ablaze by grieving family members who refuse to accept that the virus was responsible for their loved ones’ deaths. Last week, a harrowing incident saw a group of young men storm a hospital in eastern Congo to retrieve the bodies of two relatives. During the ensuing chaos, CNN reported that 18 individuals suspected of having Ebola fled the facility and disappeared. These are undeniably nightmarish conditions for effective disease containment.
However, CEPI has responded decisively, injecting $87 million into the development of three promising vaccine candidates for the Bundibugyo virus, which are currently in the early stages of testing. This “scattergun strategy,” as Halton describes it, mirrors the approach that proved successful during the COVID-19 pandemic. “During COVID, CEPI had investments in 14 vaccine candidates, of which seven got to some form of licensure,” Halton stated. “I describe this as the ‘many shots on goal’ approach.”

CEPI has emerged as a critical pillar in the global effort to combat novel and deadly pathogens. This non-profit organisation, partially supported by Australian funding, champions scientific research aimed at developing countermeasures for emerging diseases in a world increasingly prone to pandemics. Beyond funding, CEPI actively engages in disease control simulations with laboratories and governments. In one notable exercise, a University of Queensland laboratory was tasked with developing a vaccine for a hypothetical, highly contagious virus spread by pygmy rice rats within a stringent 150-day timeframe. While no actual outbreak was occurring, this simulated challenge was designed to hone the world’s capacity for rapid vaccine development. Some of these preparedness drills have proven eerily prescient.
CEPI conducted an exercise with the Rwandan government in September 2024. The scenario involved a young abattoir worker presenting with fever, joint pain, and headaches. Tragically, three healthcare workers who attended to him also became infected, with one succumbing to the illness. The exercise focused on how the government should respond. In a last-minute decision, Marburg, a severe haemorrhagic fever, was chosen as the fictional disease. This simulation proved invaluable, allowing health authorities to refine their outbreak response plans and identify potential bottlenecks that could impede rapid disease control.

Little did they know, at the exact same time, a real 27-year-old Rwandan miner began experiencing similar symptoms of aches and fever. His pregnant wife also fell ill, as did healthcare workers at the hospital where they sought treatment. It was Marburg, marking its first documented flare-up in Rwanda. Fortuitously, thanks to their recent “war game” exercise, the Rwandan government was able to mobilise swiftly. They initiated contact tracing and door-to-door surveillance, simultaneously calling upon CEPI and its partners to identify a suitable vaccine candidate. Within a mere 10 days of the outbreak’s commencement, Rwanda had an emergency vaccine trial underway, and by December of that year, the disease was brought under control.
“One of the things we’ve learnt is how to move quickly, very quickly, through all the steps necessary to go from a possible candidate through to manufacturing,” Halton explained. CEPI is actively facilitating the overlap of traditional sequential stages – basic science, animal studies, human trials, peer review, regulatory approvals, and vaccine manufacturing. This streamlined process aims to ensure that if a vaccine proves successful, it can be deployed with unprecedented speed.

“If you do all of that in parallel, you shrink the time very significantly. CEPI has an understanding of all of this ecosystem, everything from the bench science all the way through to how you get a product produced and moved into a country,” Halton elaborated. “It’s getting rid of what I describe as the ‘white space’ in the timetable. There are no corners cut – it’s scientifically robust,” she emphasised. While this approach carries the inherent risk of financial loss if a candidate fails, Halton views it as a necessary investment. “If you want to save money, you spread everything out, you do it one at a time, and you don’t invest more money until the answer is very clear. But that takes a long time. We want access, and we want speed,” she asserted. “If it costs more money, we don’t care – well, we do care, but we think that that is a premium the world should pay to actually get something that works.”
The world currently lacks a definitive response to Bundibugyo, despite its deadly potential, partly due to its rarity, which makes it commercially unviable for many developers. This is precisely why CEPI has committed $87 million in “push” funding to accelerate the testing of new vaccine candidates. Concurrently, Gavi, the Vaccine Alliance, has allocated $40 million (approximately $57 million AUD) in “pull” funding to bolster production capabilities even before a vaccine’s efficacy is fully confirmed. This integrated “push-pull” strategy is designed to mitigate the financial risks undertaken by developers during the testing phase while simultaneously ensuring that safe and effective treatments reach the front lines as rapidly as possible.
CEPI has invested $50 million (US) into the preclinical testing and clinical trials for a Moderna Bundibugyo ebolavirus vaccine candidate. This funding also covers the manufacturing of sufficient doses to enable immediate large-scale Phase 2 and 3 trials should Phase 1 prove successful.
An additional $3.2 million (US) has been directed towards an IAVI candidate engineered to induce rapid-onset immunity. CEPI is also expediting the development of a third vaccine option, allocating $8.6 million (US) for a project utilising the University of Oxford’s ChAdOx1 platform. This innovative method employs a weakened chimpanzee adenovirus, the cause of the common cold, to deliver harmless fragments of the Bundibugyo ebolavirus, thereby stimulating an immune response. This same platform was instrumental in the development of the AstraZeneca COVID-19 vaccine, which was administered to billions during the pandemic. The WHO anticipates that human trials for the Ebola-specific version could commence within two to three months.
Jane Halton is actively campaigning for $2.5 billion in funding for CEPI 3.0, a comprehensive five-year pandemic preparedness plan. This initiative aims to develop treatments capable of combating entire families of viruses, rather than focusing on individual pathogens. The goal is to equip the world with the ability to design and distribute new vaccines within 100 days, well before the emergence of “disease X,” the next global health crisis. Halton estimates that such rapid response capabilities could have saved approximately 8 million lives during the COVID-19 pandemic. “It’s about speed, safety and scale to save lives,” Halton stated. “That’s what we’re trying to do.”